
NHS London are investing in strategies aimed at increasing uptake of cervical cancer screening and HPV vaccination, but they needed the evidence to show the impact that these services will have. The organisation commissioned the Health Economics Unit (HEU) to demonstrate the benefits of investing in ways to achieve cervical cancer elimination, from a health care and wider societal perspective.
An ambitious drive to reduce cervical cancer prevalence
Cervical cancer remains a significant public health issue and is a highly prevalent disease in women, particularly those under the age of 45 and immunocompromised. There are around 3,300 new cases and 850 deaths per year in the United Kingdom (2017-2019) – making it the fourteenth most common cancer in the UK.
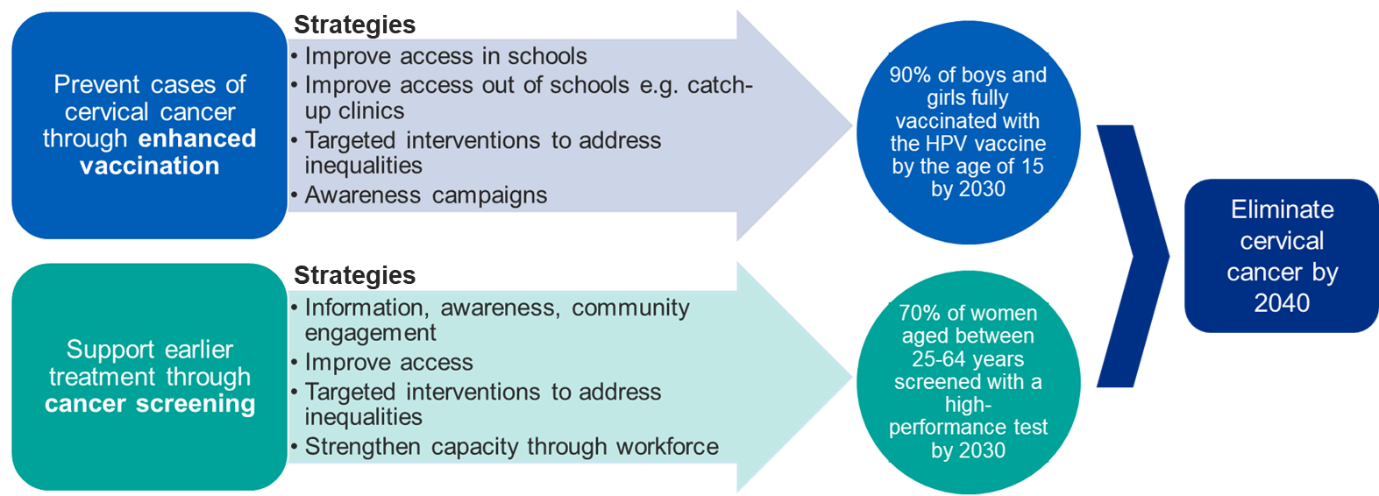
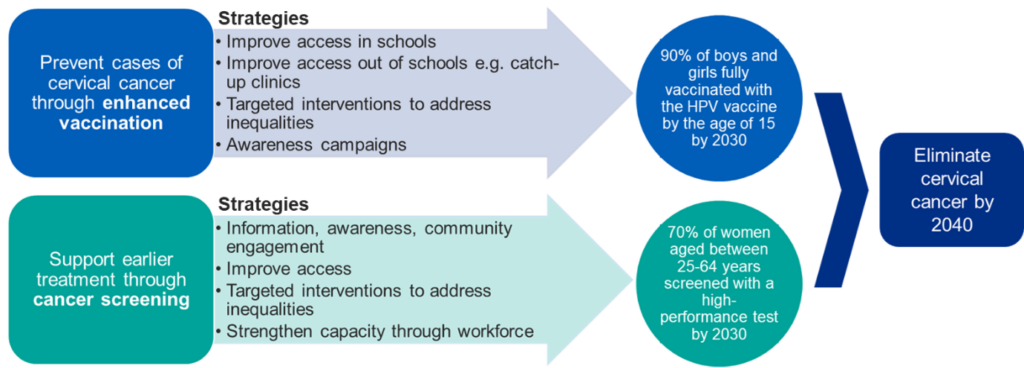
In 2023, NHS England set an ambition to achieve the World Health Organisation (WHO) cervical cancer elimination target of 4.0 cases per 100,000 population by 2040. This aligns with the NHS’s overarching goal to improve prevention and drive earlier cancer diagnosis. The ambition to eliminate cervical cancer also reflects NHS England’s commitment to delivering value-for-money public health interventions and boosting economic productivity.
Understanding the data behind interventions
The HEU carried out modelling to estimate the economic gains of achieving HPV vaccination and screening coverage targets, from the perspective of the health care system and wider society.
The team adopted a dual approach to capture not only the return on investment but also the health gains by combining a cost-benefit analysis (CBA) with a cost-effectiveness analysis (CEA).
The primary outcomes were net present value (NPV) and incremental cost-effectiveness ratio (ICER). Secondary outcomes included the life years gained, quality-adjusted life-years (QALY) gained, cost savings, and monetary benefits.
To estimate outcomes, the HEU developed an adaptable, multi-year decision tree (2025 to 2050) in Excel. The model examines the effect of HPV vaccination and cervical screening on the incidence of cervical intraepithelial neoplasia (CIN) and cervical cancer, and associated costs and outcomes, among women aged 25 to 64 living in London.
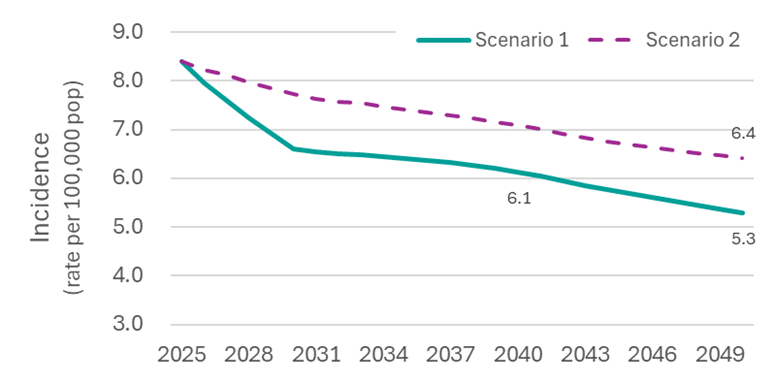
The team compared two different scenarios in the model: i) Best case – HPV vaccination and screening coverage rates are achieved, and ii) HPV vaccination and screening rates remain the same.
The case for investment
The results of the HEU’s modelling showed the following conclusions:
Investing in prevention pays off over time
There is cost to preventing and treating cervical cancer but investing in prevention pays off over time, both economically and in terms of health outcomes. Over 25 years, this investment is estimated to result in a cost saving of £113.4 million in NPV terms, and a greater health benefit, with 6,490 QALY losses avoided compared to the baseline.
Investing in prevention reduces cervical cancer incidence and saves lives
The long-term impact of increased vaccination and screening in Scenario 1 (best case) results in fewer cervical cancer cases overall, with the greatest reduction seen in early-stage diagnoses.
However, the NHS England elimination target (≤4 cases per 100,000 by 2040) looks unlikely to be reached within the modelling period. This may partially reflect conservative assumptions around vaccination coverage.
Investment results in economic gains to the wider economy
In terms of societal costs and benefits, productivity losses are consistently lower under Scenario 1 (best case) compared to Scenario 2, reflecting fewer cases of cervical cancer and associated morbidity and mortality. These findings suggest that increased investment in vaccination and screening can lead to measurable gains for the wider economy by keeping more individuals healthy and economically active.
Financial costs to health care system are offset somewhat by reduction in treatment costs
The overall cost to the healthcare system (vaccination, screening, diagnosis and treatment) is similar in both scenarios. However, the savings to the healthcare system is underestimated in the HEU’s model since
i) the financial gains from vaccination will continue to accumulate far beyond the timeframe of the model and
ii) it does not account for other HPV-related cancers, such as oropharyngeal, anal, or vulvar cancers.
Evidence suggests that 80% of total cancer-related QALY gains and cost savings from HPV vaccination (in a UK context) are attributable to cervical cancer, with the remaining ~20% attributable to other anogenital cancers.
Planning to save money and save lives
The HEU’s work provides economic evidence of the benefits of investing in prevention and early detection, demonstrating that investing in initiatives to increase HPV vaccination and screening coverage saves money and saves lives.
The modelling offers a replicable approach for other regions and ICSs aiming to contribute to national cervical cancer elimination goals.