
As the North East London Critical Care Transfer And Retrieval (NECCTAR) Service approaches the end of its first year of operation, the country is once again facing a COVID level 4 alert and a new coronavirus variant. Jonathon Dean, Critical Care Hub doctor from Barts Health NHS Trust and member of the NECCTAR hub, explains how the learnings from 2021, made in conjunction with colleagues from the Health Economics Unit, will help support the local response.
NECCTAR was formed in 2020 to help critical care units manage the large influx of COVID patients by providing an additional resilience layer for intensive care provision. The aim was to preserve the standard of critical care support whilst transitioning patients across intensive care units in the sector, the London region, and nationally.
We were fortunate to have had input from the analytics and health economics teams at the Health Economics Unit (HEU) from the very start, guiding the data capture and analysis within our services and other linkable sources including the North East London Critical Care Hub. Their use of real-world data has been vital to our work in making a real difference to critical care within the NHS.
We initially supported critical care units to decompress by transferring patients as needed to alternative sites, ensuring no single facility was overwhelmed. We have since expanded the service’s scope and capabilities, aiming to progress the subspeciality of retrieval medicine.
As I write in mid-December, we are expecting yet another wave of COVID driven by record numbers of the new omicron variant; parliament has just voted for some restrictions to be reintroduced with the potential for more to come, and there’s a huge drive within the NHS to give as many booster vaccinations as possible by the end of the year. The work of our team to develop the right support for the sharp end of care couldn’t be more important right now.
About NECCTAR
Over the last year, NECCTAR has received referrals for 583 patients (including some for advice only), and we successfully transferred 505 people with excellent outcomes. The team has travelled 10,000kms with critical care patients, ensuring a safe journey and efficient load balancing.
Starting at the height of the second wave, we captured daily real-time data from every one of our sector’s intensive care units that allowed us to predict demand for critical care and transfers. Since then, the marriage between our data and powerful analysis in health economics has enabled our service to reach some real heights and to expand into other areas of critical care.
We have developed the service from being a primarily decompression service of necessity into a 50/50 split for clinical and non-clinical moves, including some where patients need to access clinical services at another site, for example neurosurgery following a major trauma, or specialist cardiac care following a heart attack or injury such as a stabbing that need constant blood pressure and respiratory support from a critical care team.
We are now in an excellent position to scale up the service for any future critical care capacity crisis, maintaining the skills we and the transfer teams need.
Deciding when we need to scale up
Demand for ICU related transfers varied with the waves of the pandemic and NECCTAR has scaled to the needs of the sector. A second NECCTAR team was made available for a 47-day period from 12 January to 28 February, during which time we were tasked 138 times, for an average of 2.9 transfers per day, with around 80 per cent related to COVID patients.
As a team, we have now harnessed the power of data to generate a threshold model for scaling our service in anticipation of sector demand, using a retrospective analysis of our activity around the time that our second team was active so as to create a prospective plan for triggers and thresholds for potentially doing so again in future surges. Standing up a second team comes with a direct cost as well as opportunity costs.
A variety of variables was considered, explored and retrospectively modelled to attempt to identify a threshold that matched our reactive decision to stand up and, eight weeks later, stand down a second crew – and this is where having data wizards capable of separating the signal from the enormous amount of noise is really crucial. Anyone with access to an electronic health record is essentially drowning in data noise, and that’s even before incorporating each unit and sector’s unique geography and demography – where do you even start?
Our data collection, modelling and real-world observation showed that a threshold of 12 critical care patients per 100,000 population is needed to trigger the deployment of the second NECCTAR team (figure 1). In early 2021, the second team was maintained for an additional week after the rate fell below the threshold to assist with repatriations and the closing of surge beds. This ensured the allocation of resources was data-driven.
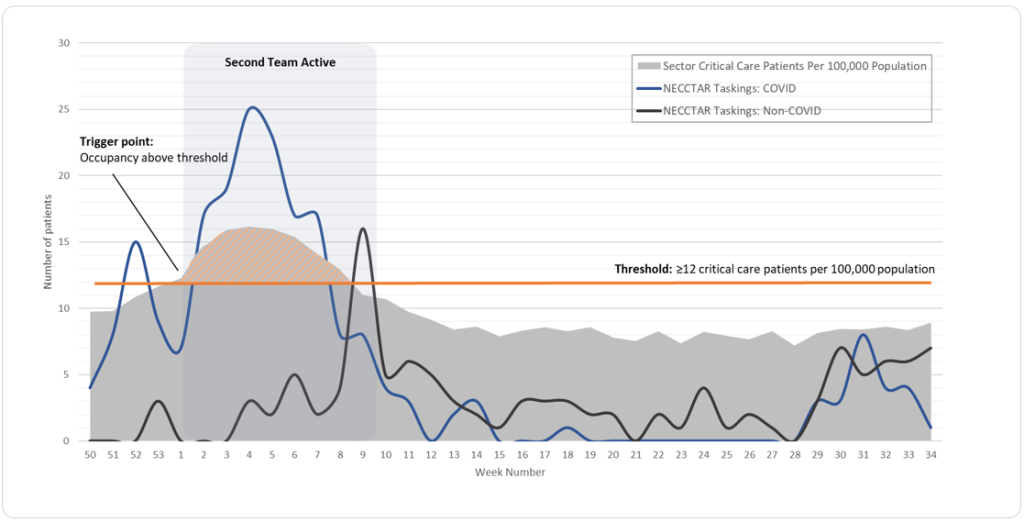
Figure 1: A data-led analysis of the threshold for additional NECCTAR deployment
As at the end of November 2021, the rate of critical care patients per 100,000 population stood at 9 per 100,000; however, I do expect us to reach at least close to 12 again over the winter, especially if the worst-case scenario predictions around the omicron variant prove to be accurate.
Our excellent data analysis support means that we will be able to back up decisions with data, using real-world data modelling that can rapidly generate hypotheses for clinicians to test out what they can do. For example, our live dashboard for occupancy and transfers means teams can look at options such as increasing equipment like ventilators that will allow them to hold their nerve and remain within capacity before considering transfer options.
The importance of real-world data analysis
Using real-world data, we can proactively move to decompress a situation before it becomes unsafe. We receive a regular flow of information about the sickest patients in the region and this information is processed, analysed and discussed locally to agree patient movements, load-balancing and safety.
The importance of such real-world, real-time data was reflected in The Economist this October, which says that “the world is on the brink of a real-time revolution in economics, as the quality and timeliness of information are transformed”.
The article discusses how many official figures that economists track come with lags of weeks or months. It argues that the promise of ‘instant economics’ is transformative, supporting better, timelier and more rational decision-making.
NHS England CEO Amanda Pritchard is also quoted as saying that “A good analyst can save more lives than a good anaesthetist”. While it’s great to see the importance of data analysis recognised, we mustn’t work in silos and it’s important that those in clinical and data roles work together, understanding what each discipline can bring to the other, with an overall benefit for us all.
Fast analysis
The piece in The Economist highlighted how novel data and its fast analysis is now being used in health and more broadly for pandemic disruption. NECCTAR is an excellent example of how data can be leveraged if separated from the noise – working in partnership with the specialist health economists and analysts who can identify which signal in the data is most likely to be relevant.
Within the NHS there is a historic, almost ‘dinosaur-like’ hesitancy to use rapidly generated data, and a level of risk aversion. However, in fast-moving situations and with the prime minister declaring an ‘omicron emergency’, this way of working with novel data analysis and data-driven responses is becoming ever more important
Jonathon works in partnership with the Health Economics Unit (HEU) and together with colleagues he took an abstract to the Intensive Care Society’s State of Art virtual event in December. Find out more at https://soa.ics.ac.uk/programme/, For more information, follow the NECCTAR team on Twitter or go to https://www.necctar.net/ . Find out more about the HEU at /